

Why do DANCERS get HIP PAIN?
We have covered knee anatomy and ankle/foot anatomy when discussing dance injuries, our next body part we are going to discuss is the hip! The hip is even trickier than the knee and ankle, but if we focus on the anatomy, it will help you figure out what is involved with your injury!

Gluteus Medius
GLUTES
We have three glute muscles. Gluteus medius and minimus do a very similar job (abduction and pelvic stabilization when standing on one foot). They also contribute to some internal rotation. Your gluteus maximus externally rotates, and is at its greatest mechanical advantage when extending the hip from 90 degrees of flexion, no abduction. Our glutes can refer pain down our thigh to our knee so they should always be investigated with hip or knee pain.
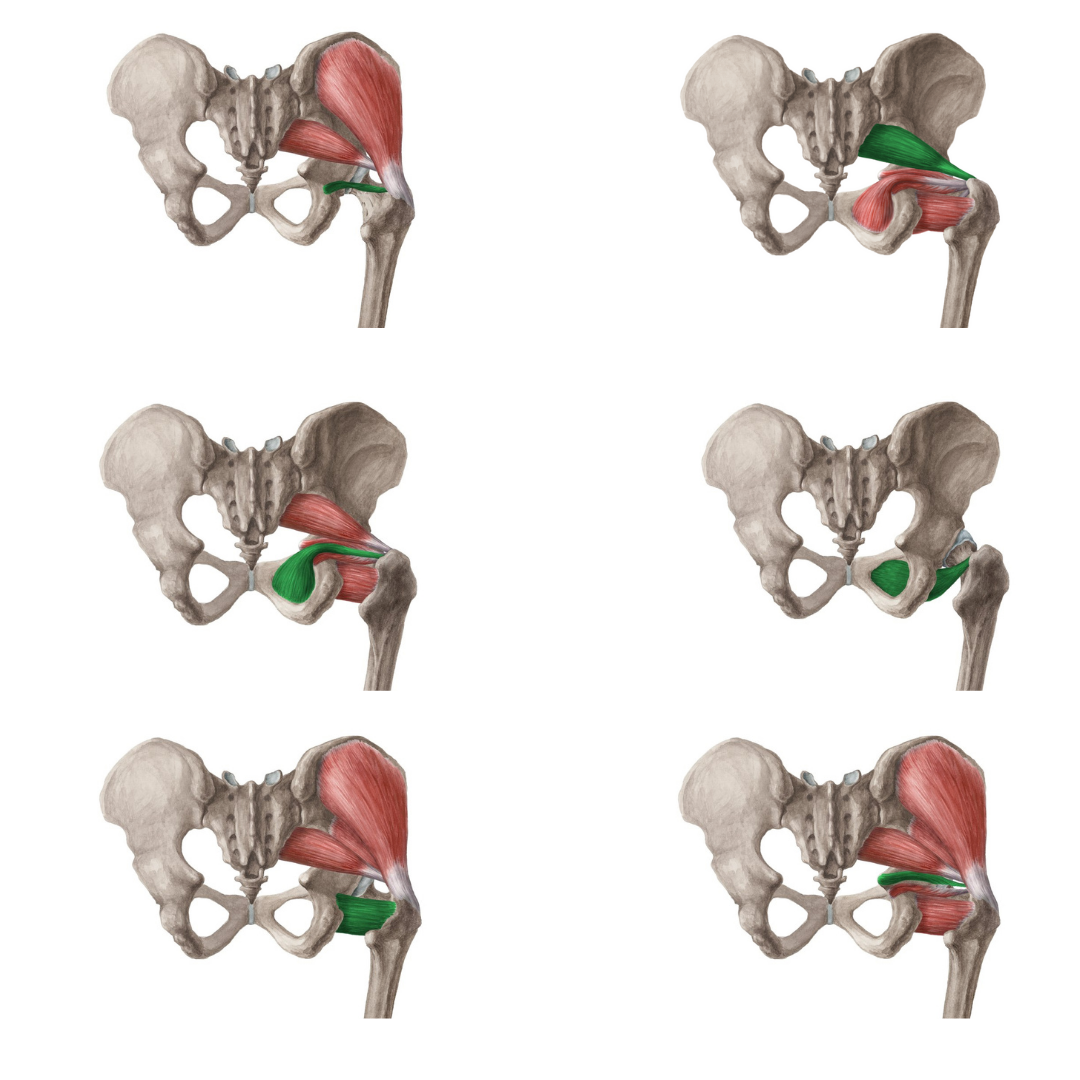
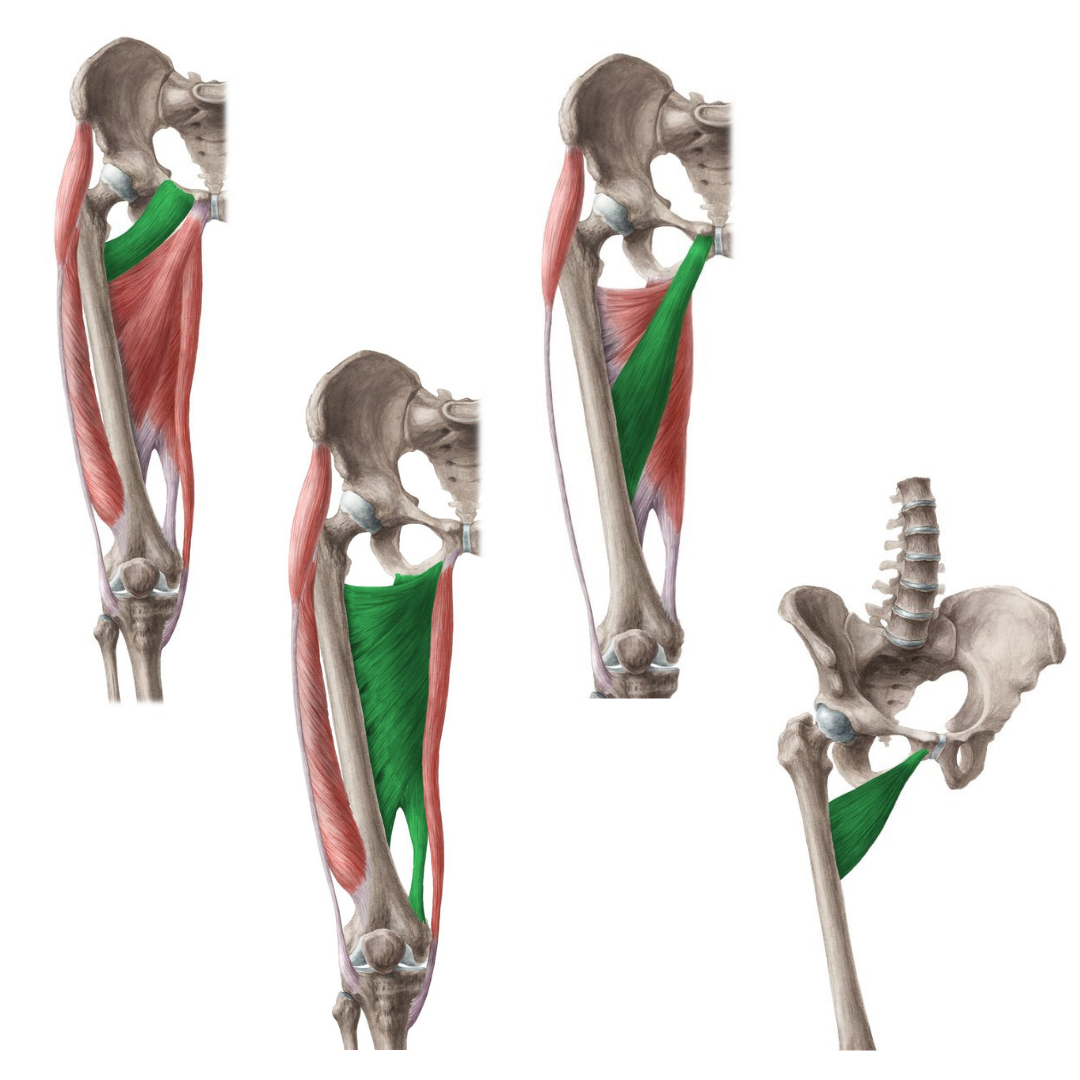
Deep Six External Rotators
PIRIFORMIS
Our piriformis is one of our deep 6 external rotators. The other 5 are quadratus femoris, gemellus superior, gemellus inferior, obturator internus and obturator externus. These muscles are responsible for so much of classical ballet movement as it is performed externally rotated for the most part. Not only do these muscles refer pain around the hip, but the sciatic nerve passes underneath piriformis, meaning it can become entrapped by tight and hypertonic musculature.

Sacroiliac Joint
SI JOINT
As our upper body weight passes into our pelvis and into our legs it passes through a joint between your sacrum and your ilium. Your sacroiliac joint is synovial but it does not move much. When this joint is irritated or the ligaments around it are sprained it can be quite painful although usually quite easy to pinpoint the area of pain by the patient (PSIS).
LUMBAR SPINE
Because the lumbar spine is involved in most motions that involve hip flexion or extension, the lower part of the spine can contribute to the hip pain you are feeling. In our spine there are joints, discs, and many ligaments and joint capsules that can become irritated causing hip pain.
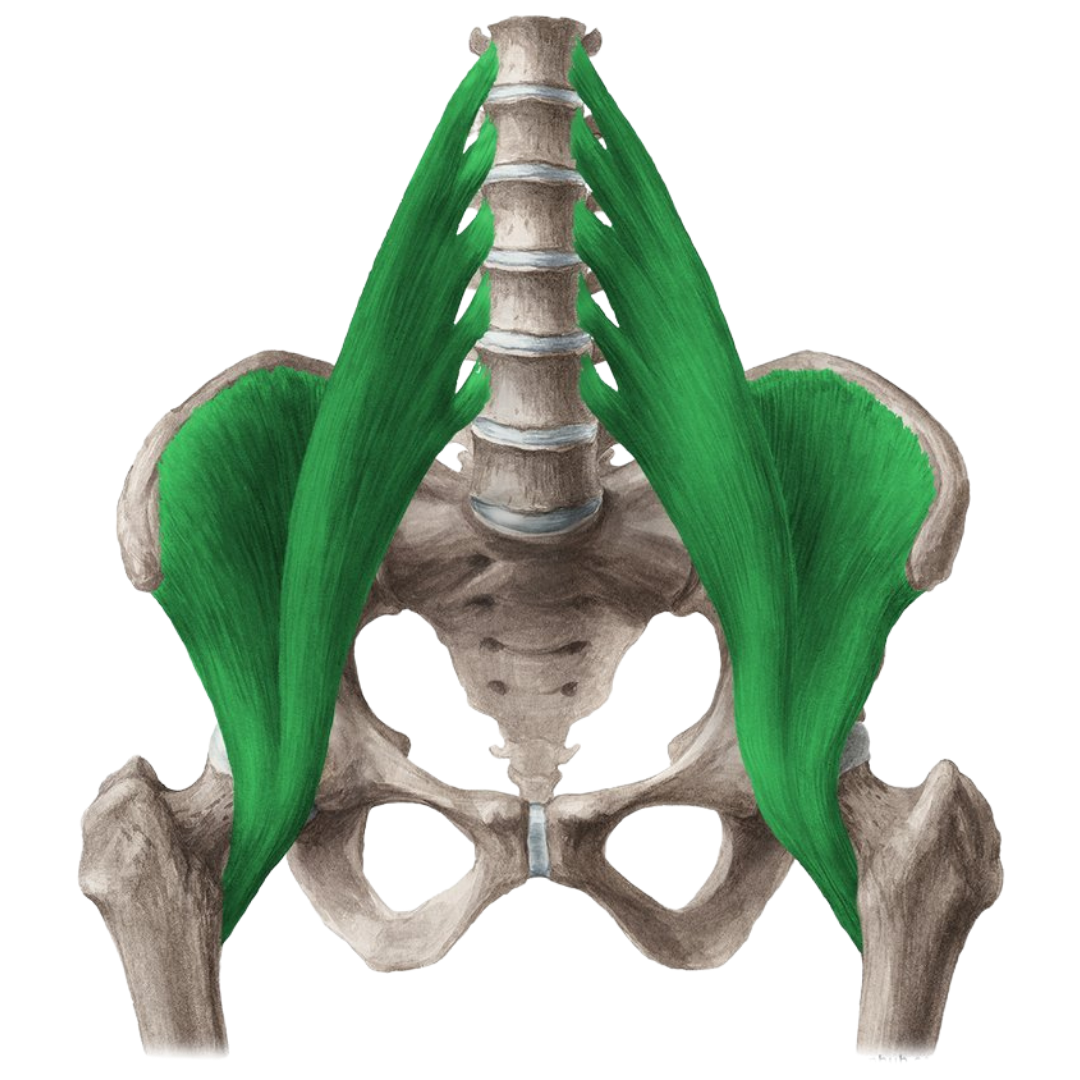
Iliopsoas Muscle
PSOAS
Our psoas attaches to the bottom of our spine, joins with iliacus, crosses the hip joint and attaches distally on the lesser trochanter of the femur (upper inner thigh). This muscle is one of the main hip flexors and when it gets inflamed can make a snapping sound and cause hip pain. For dancers, this is a very easily overworked muscle.
LABRUM
Our labrum is the cartilage that sits in our hip socket (acetabulum). When this cartilage is damaged or torn it can also make a clicking sound like psoas, can be quite painful, and can lead to early degeneration (osteoarthritis).
ACETABULUM
As mentioned above, our hip socket or acetabulum can be part of the reason we are experiencing hip pain. Another reason beyond the labrum being damaged is how deep or shallow the acetabulum is itself. One condition typically caught at birth is Congenital Hip Dysplasia. This condition is where the acetabulum is very shallow. This can lead to more dislocations and early degeneration (ie. early hip replacement).
ASIS/AIIS
Your ASIS and AIIS are the bony site of attachment for your hip flexors. If we are doing a sport with a lot of kicking or hip flexion (soccer, gymnastics, dance), we can have pain from this area. If it is before the growth plate located here is fused, then it is considered a Salter-Harris type fracture. If it is after the growth plate has fused, then it is considered an avulsion. Either way, this can be seen on radiographic imaging and should be included in a differential list about hip pain.
CAPSULE
Think of your capsule as a sock around your hip that adds passive stability. Our capsule can become inflamed and then tight. Most dancers hit a hip capsule stretch at some point in their warm-up, but if you need guidance, consult a licensed healthcare professional.
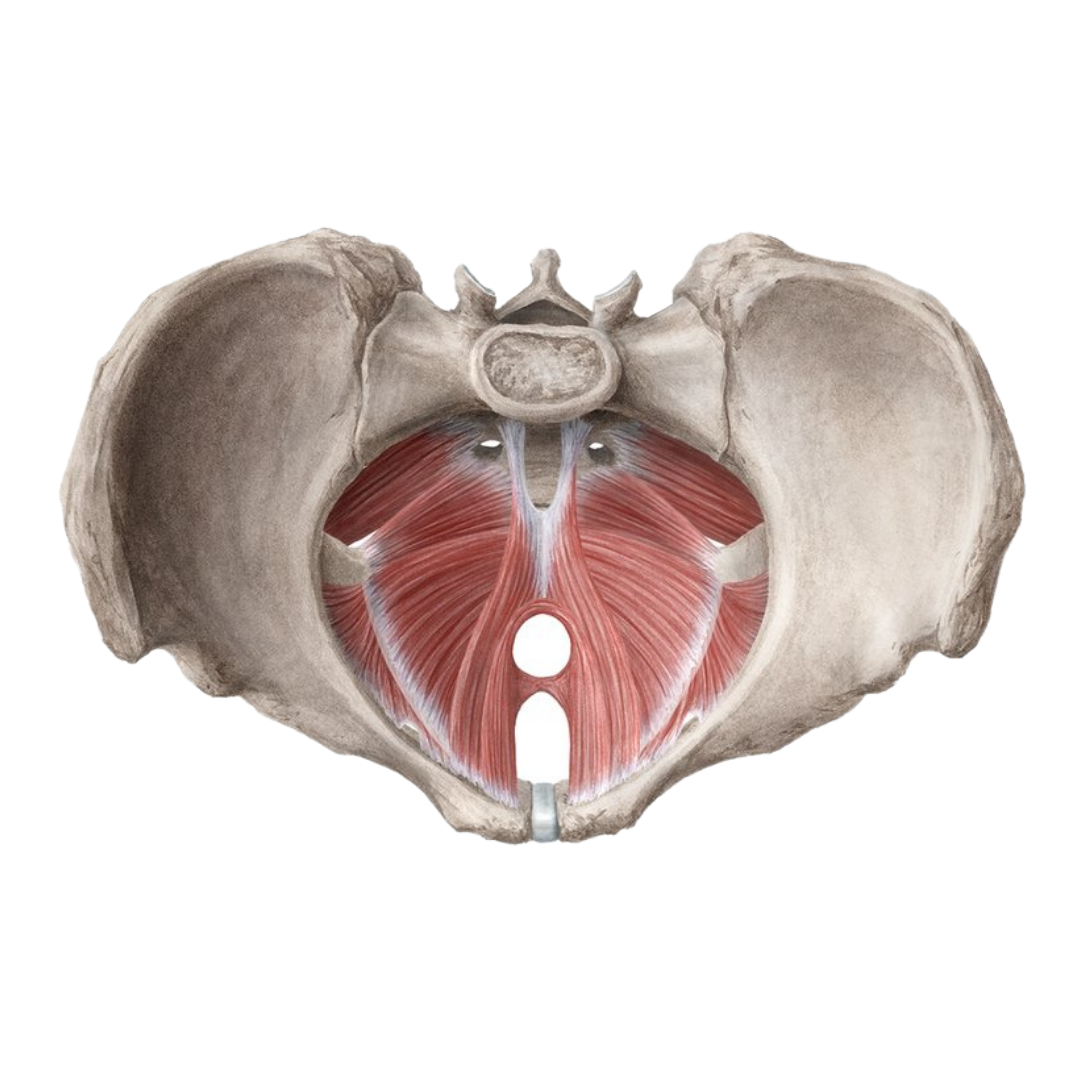
Pelvic Floor
PELVIC FLOOR
Think of the pelvic floor as the bottom of the core. Think of your core as a pop can. Your core has is three dimensional with a top (your diaphragm) and a bottom (your pelvic floor). As oblique muscles join distally into this ‘core’, there can be tension, or pulling in the anterior hip region all due to an overactive pelvic floor and oblique muscle. You may want to consult a pelvic floor physiotherapist if you are experiencing hip pain and not seeing any results with manual therapy.

Quadratus Lomborum
QL
Your quadratus lumborum or QL attaches to your pelvic crest and your bottom rib. This muscle extends your spine, laterally flexes your spine, and fixes the bottom of your rib cage during inspiration. Our QL is the muscle just proximal to our glutes so you can see how QL can play many roles in hip pain. QL can also refer pain intake hip area so it should always be checked out when experiencing hip pain.
Tensor Fascia Latta
TFL
Tensor Fascia Latta or TFL is a muscle that has already been mentioned. TFL runs between your ASIS and your IT band and it is a lateral hip stabilizer. It also plays a role in tightening the IT band and knee mechanics. Because TFL is so intimately involved in hip mechanics as well it is another muscle that can contribute to hip pain.
FEMORAL HEAD
The top of your femur has an angled component which then finished in a round shape. This round shape is called the femoral head. Before the growth plate fuses in the femoral head, you can get slippage called Slipped Capital Femoral Epiphysis (SCFE). Typically SCFE is more common in heavier children and refers pain to the knee, but should still be included in a hip differential list. When the femoral head lacks proper blood supply, our bony tissue can die off (necrosis). If this occurs in a child it is referred to as Legg-Calves-Perthes and in an adult it is called Avascular Necrosis of the femoral head. As you can see the femoral head is an important part of the overall hip anatomy.
HIP JOINT SYNOVIAL FLUID
The lubricant in our hip joint is called synovial fluid. There is a condition where this fluid can become inflamed causing pain for a short, temporary amount of time. When this occurs it is called Transient Hip Synovitis. This typically occurs in children ages 3-10 and is the most common cause of acute hip pain in this age range.
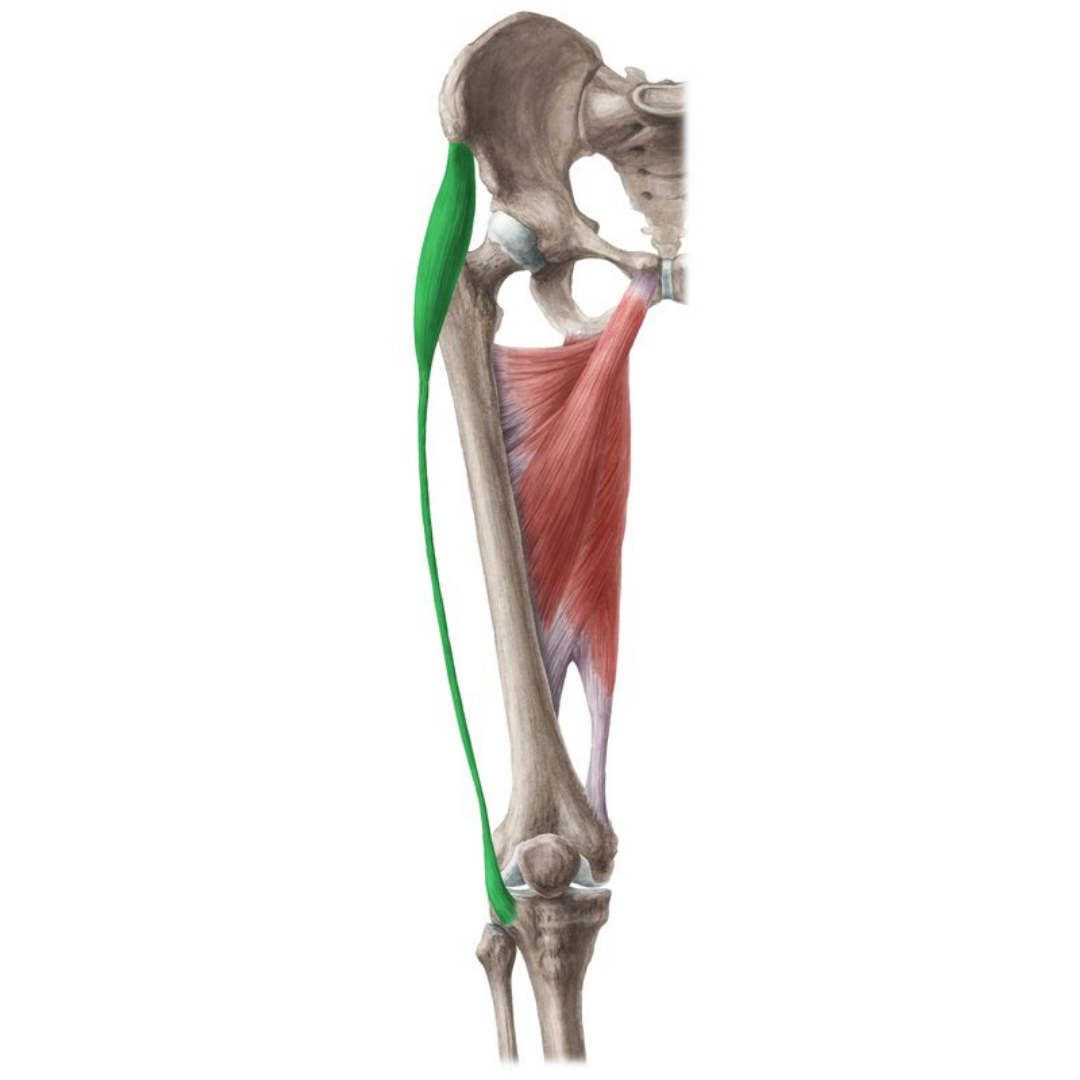
Adductors
ADDUCTORS
Our adductors include pectineus, adductor brevis, adductor longus, adductor magnus, and gracilis. When we strain one of these muscles or tear closer to the tendon, it is referred to as a groin strain/pull. Sometimes dancers can over train certain muscles, neglecting others. Once these neglected muscles we should add to our conditioning program as dancers are your adductors or inner thigh muscle. For all of these reasons, your adductors are another part of your hip anatomy important to investigate when experiencing pain.
As you can see, hip pain can be complicated and involve several anatomical components. Ensure you are seeing a licensed healthcare professional who has a knowledge in dance, better yet a personal background as a dancer.