

Growth Plate Injuries
Bone growth and maturation takes years to complete. Bones start to ossify during embryonic development, and can take until she 25 to fully complete. All bones are derived from embryonic connective tissue (mesenchyme) and ossification occurs directly ti mesenchyme or through cartilage that is also derived from mesenchymal tissue. The latter is how long bones grow.
Long bones grow by developing a cartilaginous bone model. This cartilage slowly calcifies as the bone grows in length, leaving behind bone where cartilage once was. We have primary ossification centres located in the shaft of bones which eventually is labeled the diaphysis. Secondary ossification centres are located in other parts of the bone. The centres located at the end of long bones are called the epiphysis. Secondary ossification centres located in the non weight-bearing part of the bone are called apophysis. An apophysis is the site of a tendon or ligament attachment. The area between the epiphysis the diaphysis is the called the metaphysis. This metaphysis is the area of growth for long bones. Each epiphysis or apophysis fuses at various ages. The epiphysis should not fuse until the bone reaches adult size. During the years of long bone growth, this area of growth is called your epiphyseal plate or growth plate. Injuries, infections, or malnutrition can affect growth plates leading to growth arrest, asymmetry between bones, and further complications down the road. Disease may cause either early or delayed fusion.
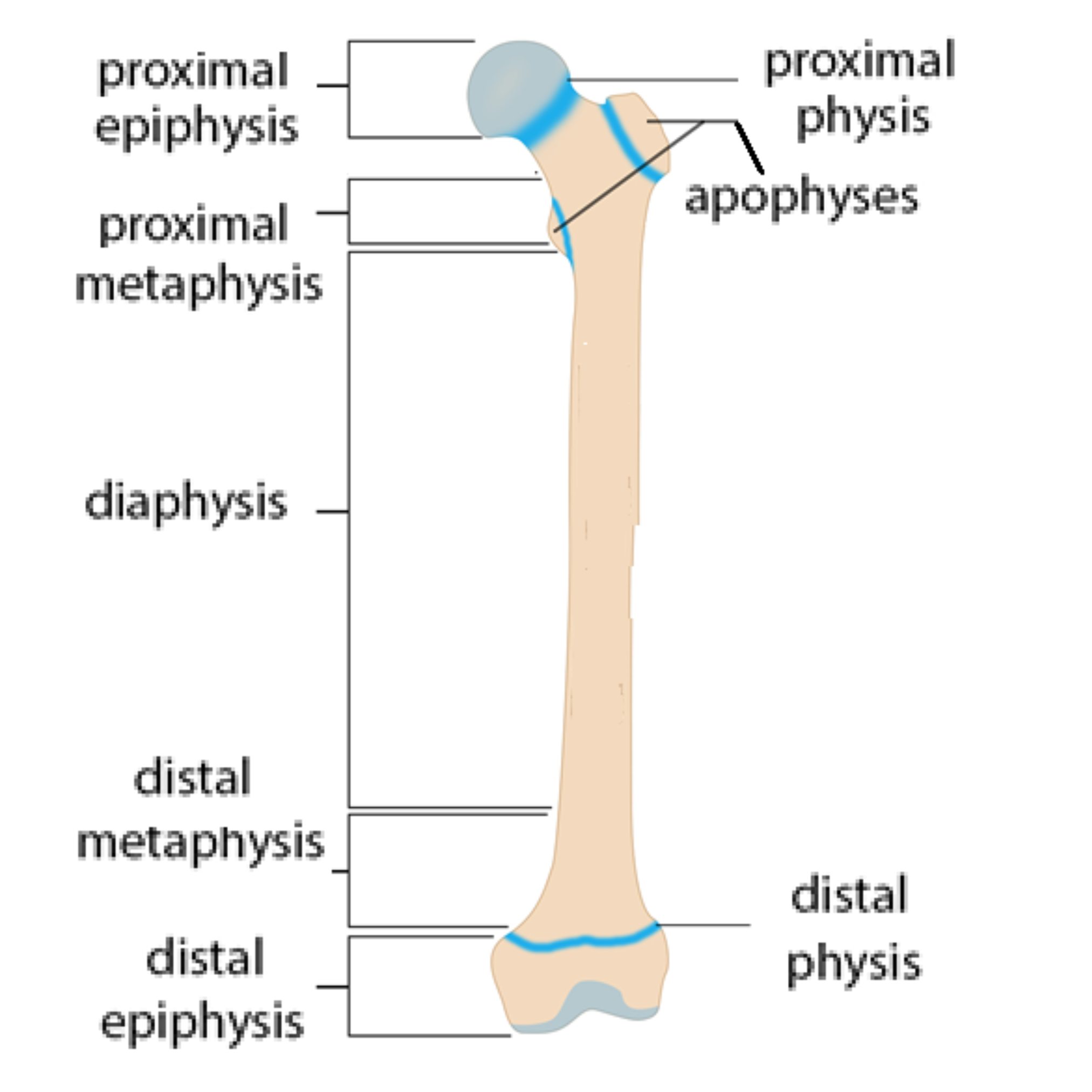
Long bone anatomy
There are several kinds of fractures and conditions related to the growth plate. Growth plate injuries can involve compaction, separation or actual breaking (fracture) around the growth plate. These fractures are called Salter Harris fractures and the type can alter both treatment and prognosis.
Let’s examine several types of growth plate injuries by body region:
SHOULDER:
Os Acrominale (Bipartate Acromion)
Incomplete fusion of secondary ossification centres caused by direct blow or repetitive overhead activity can lead to incomplete fusion (typical fusion is by age 22) resulting in rotator cuff irritation as well as inflammation. Treatment often involves activity limitation and progressive strengthening. Surgical intervention may be considered.
Acromial Apophysitis
The ossification centre is normal, but repetitive traction of the growth plate leads to pain felt in the shoulder. Typical fusion occurs by age 19. Treatment may include rest, modification of activity, and potentially adding padding to the shoulder in contact sports. Monitoring for potential nonunion of the growth plate should be included in management.
Coracoid Apophysitis - before age 21
Repetitive stress from activities like swimming, tennis, and pitching may cause traction at the growth plate at the coracoid process (where pectoralis minor, coroacobrachialis, and biceps brachii attach). Usually this growth plate fuses by age 21. Typically activity modification will suffice in most cases.
Little League Shoulder
Seen more commonly in young baseball pitchers and catchers where repetitive stress is placed on the proximal humeral growth plates. Patients should be examined for potential fracture of a bone cyst. Healing may take up to 6 weeks of rest.
Sprengel’s Deformity
During fetal growth, if the mesenchymal tissue of the shoulder blade does not migrate, there may be congenital elevation of said shoulder blade. This is usually only on one side of the body and may be treated with soft tissue release or potentially surgical intervention depending on the severity.
ELBOW:
Little League Elbow
As seen in young pitchers, distraction medially and compression laterally during the cocking phase, followed by quick pronation can lead to pain in the elbow joint. Osteochondritis dissecans (fragmentation of bone) may also be present. Early detection and strict adherence to Little League pitching rules can be helpful.
Olecranon Apophysitis
Repetitive throwing can lead to posterior elbow pain with resisted extension. Rest and activity modification with icing and stretching typically resolves this issue.
WRIST:
Distal Radial Epiphyseal Injury
Injury to the growth plates in the wrist (the end of your forearm bones) can be the result of falling onto your wrists or a twist of the wrist while bearing weight (such as gymnastics). Radiographic imaging can differentiate between growth plate injury and soft tissue injury and be used in follow up examination to ensure normal bone growth.
HIP/PELVIS:
Slipped Capital Femoral Epiphysis
Typically no mechanism of injury related, this is where there is slippage (posterior or inferior) of the growing plate at the femoral head. Common in tall, rapidly growing children, and obese children. Pain may refer to the knee and cause a limp. Orthopaedic consult should be sought out for management.
ASIS Apophysis
Sudden contraction of sartorius with hyperextension of the hip with knee flexion (sprinting position) can lead to a snapping sensation and then pain at the front of the hip with passive hip extension and active hip flexion. Palpation of an avulsed fragment may also be possible. Initial rest and ice is most important followed by use of crutches and activity modification. Radiographic imaging may help with consideration of surgical intervention.
AIIS Apophysis
This apophysis appears between ages 13 and 15 and fuses between 16 and 18. This injury is similar to ASIS, but due to over contraction of rectus femoris, commonly found in sprinters and activities with kicking, like dance. Radiographic imaging and conservative care is recommended
Lesser Trochanter Apophysitis
This apophysis appears between ages 8 and 12 and fuses around ages 16/17. Forceful contraction of iliopsoas, often against resistance (sprinting or kicking). Leg may appear in adduction/internal rotation, and feel painful with passive extension and resisted flexion. With conservative care, this may take up to 12 weeks for full recovery.
Greater Trochanter Apophysitis
This apophysis appears around age 4 and fuses between the ages 16 and 18. This injury is typically caused by sudden or repetitive contraction of hip abductors (a quick and forceful change in weight, cutting). Standing on one leg may be painful. Radiographic imaging is recommended to examine fragment displacement with possibly surgical fix if displaced enough.
Iliac Crest Apophysitis
This apophysis appears around ages 12 to 15 and fuses between the ages 18 and 25. Repetitive pulling of obliques, tensor fascia lats, gluteus medius, gluteus maximus, or latissimus dorsi can lead to pain and tenderness with abduction of the hip, abdominal muscles or lateral bending. Conservative care is recommended in most cases.
Ischial Tuberosity Apophysitis
This apophysis appears between ages 14 and 16 and fuses between 18 and 25. Excessive eccentric contraction of the hamstrings with knee extension often found in runners, jumpers, and gymnasts can lead to pain locally and with hamstring contraction. Radiographic imaging should be used to ensure full union of the growth plate.
KNEE:
Osgood-Schlatter’s
Typically around the ages of 11 to 15, this affects the apophysis located at the tibial tubercle. More common in activities involving jumping or running, like dance and gymnastics. Conservative care including activity modification, icing, strategic stretching and strengthening resolved most cases.
Sinding-Larson-Johannsen Syndrome
Occurring typically ages 10 to 14, this involves the apophysis at inferior portion of the patella (kneecap). Similar causes to Osgood-Schlatter’s, climbing stairs and kneeling may be particularly painful in this case. Care and prognosis is similar to Osgood-Schlatter’s.
Epiphyseal Injury
An injury involving hyperextension, twisting, or buckling at the knee may be more likely to affect the growth plate than the soft tissue. Growth plate fractures should be investigated using stress fluoroscopic radiographic study.
FOOT:
Sever’s Phenomenon
This affects secondary ossification centres in the calcaneus. More common in boys, pain is worsened with running. Tight gastrocnemius/soleus, and previous injury, weak dorsiflexors (tibialis anterior), genu varum (knock-kneed), and forefoot varus can predispose children. Swelling is rare. Conservative care is recommended.
Iselin’s
In this condition, the growth plate on the outside of the foot at the base of the fifth metatarsal is tractioned. Running, jumping, and cutting sports are more associated. Resisted eversion of the ankle may cause pain. Stretching and evertors and plantarflexors and strengthening the dorsiflexors and investors is recommended.
As always, consult a licensed healthcare practitioner if you are experience pain or issues with activities.
REFERENCE LIST:
Souza TA. Differential diagnosis and management for the chiropractor: protocols and algorithms. Jones & Bartlett Publishers; 2009 Oct 7.